Key takeaways:
IUDs (intrauterine devices) and implants are the most effective birth control alternatives that aren’t the pill. These are also called long-acting reversible contraception (LARC).
Hormonal contraception can help with cramps and make periods lighter.
Combined hormonal contraceptives (estrogen and progestin) raise the risk of blood clots. But they also have some benefits, like a lower risk of some cancers.
Progestin-only contraception options are safe after giving birth and while breastfeeding.
There are also natural and nonhormonal birth control options, such as fertility awareness and withdrawal methods.
The most common types of birth control are surgical sterilization (such as “getting your tubes tied”) and birth control pills (“the pill”) — and for good reason. They’re very effective. But they’re not for everyone. Sterilization is convenient but permanent. And the pill needs to be taken at the same time, every day, which can be tough to remember. Plus, the side effects of the pill can be hard to manage for some people.
Luckily, there are many alternative forms of birth control. There are options that you use just when you need to, like Phexxi gel or the diaphragm. Others, like IUDs (intrauterine devices), implants, and injections, involve a visit with a healthcare professional. There are also in-between options that you can insert or apply yourself every month, like contraceptive rings and patches.
With so many options, there’s sure to be a method of birth control that’s right for you.
Search and compare options
Types of birth control alternatives
There are plenty of options if you’re interested in contraception that doesn’t involve the pill or surgery. They vary in terms of ease of use, effectiveness, and length of protection against pregnancy.
Before we take an in-depth look at each one, here’s an overview of the different options:
Long-acting, reversible contraceptives (LARCs): These methods include implants and IUDs. They’re the most effective and easiest to use, and they can last for years. A healthcare professional has to place an IUD or implant, but then you don’t need to do anything afterwards. There are both hormonal and nonhormonal options.
Injections: The Depo-Provera (medroxyprogesterone) injection isn’t quite as error-proof as LARCs, but it requires less monitoring than the options you place yourself.
Patch and ring: These options contain hormones and are more convenient than a daily pill. But, in order to have your best chance of avoiding unplanned pregnancy, you need to remember to switch them out.
As needed: The cervical cap, diaphragm, spermicide, and Phexxi (lactic acid/citric acid/potassium bitartrate) are used before sexual activity. They are nonhormonal, prescription forms of birth control that require more work on your part. Generally speaking, they aren’t as effective as the other methods, so consider using them with another form of birth control. Condoms also work as-needed, without a prescription.
Just remember that regardless of which type of birth control you choose, they don’t protect against sexually transmitted infections (STIs), like gonorrhea or HIV. Only condoms can give that kind of protection.
Comparing nonpill birth control alternatives
Here’s a quick comparison of prescription birth control methods that are not the pill.
| Type | Hormones | Duration of protection | Typical efficacy |
|---|---|---|---|
| Implant (Nexplanon) | Etonogestrel | 5 years | > 99% |
| Copper IUD | None | > 99% | |
| Hormonal IUD | Levonorgestrel | > 99% | |
| Injection (Depo-Provera) | Medroxyprogesterone | 3 months | 94% |
| Vaginal ring | 1 month | 91% | |
| Patch | 1 week | 91% | |
| Cervical cap (FemCap) | None | 6 hours or more (place before sex) | 84% or less |
| Diaphragm | None | 6 hours or more (place before sex) | 83% |
| Phexxi vaginal gel | None | 1 hour (apply before sex) | 86% |
Below are more details about seven birth control alternatives to the pill.
1. Nexplanon implant
The contraceptive implant (Nexplanon) is a thin, plastic rod that’s inserted under the skin in your arm. It releases the hormone etonogestrel (a progestin), which helps prevent ovulation (release of an egg by an ovary).
It also prevents pregnancy by thickening the mucus in the cervix (where the vagina meets the uterus). This makes it harder for a sperm to reach and fertilize an egg in case ovulation does occur. It also thins the lining of the uterus, making implantation more difficult.
Benefits
There are a few benefits of the implant including:
Can help with symptoms related to endometriosis or your period
Safe to use if breastfeeding
Side effects
The most common side effect is irregular bleeding, and there’s no way to predict how or if your period will change. Other possible side effects include:
Headaches
Breast tenderness
Worsening acne
Risks
There’s an increased risk of blood clots in people who smoke. Regarding breast cancer risk, the evidence is mixed. Some research suggests progestin-only birth control such as the implant may also raise the risk of breast cancer in some people. But other studies didn’t find such a link.
You shouldn’t get an implant if you are pregnant or have:
Breast cancer (current or past)
A current or past blood clotting problem
Liver disease
Unexplained vaginal bleeding
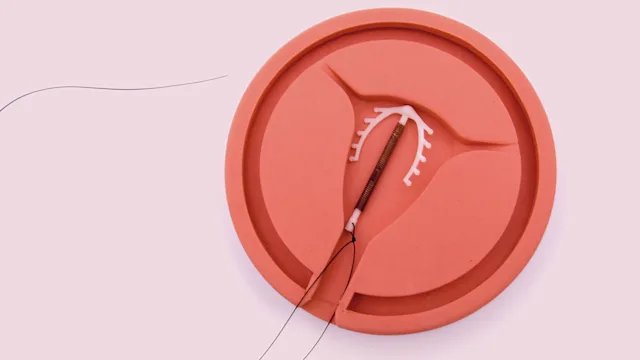
2. Intrauterine devices
IUDs are T-shaped contraceptive devices that are placed in the uterus to prevent fertilization of an egg by sperm. There are two types of IUDs: copper (nonhormonal) and hormonal. And they work a little differently.
Copper IUD
The copper IUDs (Paragard and Miudella) are hormone free. They release copper ions, which are toxic to sperm. This makes it difficult for sperm to move and enter the uterus. Miudella contains less copper than Paragard but can’t stay in as long.
Hormonal IUD
The other IUDs release levonorgestrel, a progestin. This thickens the cervical mucus, making it difficult for sperm to reach the uterus. It also helps prevent ovulation and thins the lining of the uterus.
You have a few different types to choose from:
Skyla
Mirena
Kyleena
Liletta
Getting an IUD placed
You’ll need to see a healthcare professional in a clinic or outpatient setting to have an IUD placed. This procedure lasts only a few minutes, but it’s uncomfortable and even painful.
The IUD has strings attached to it. Your healthcare team will ask you to “check your strings” about once a month. You simply insert a clean finger into your vagina, and you should feel the strings at your cervix. This is an important check to be sure the IUD hasn’t moved out of place.
If you have an IUD and want to get pregnant, or if you have side effects from it (see below), know that an IUD can be removed at any time. Simply contact your healthcare team for a quick visit.
Benefits
Possible benefits of IUDs include:
Lower risk of endometrial cancer
Lighter or no periods (hormone-releasing IUDs)
Less pain related to menstruation and endometriosis
Safe to use immediately after giving birth or having an abortion
Can be used as emergency contraception if placed within 5 days of unprotected sex (Paragard IUD)
Side effects
Possible side effects of the hormone-releasing IUDs include:
Breast tenderness
Mood changes
Headache
Possible side effects of the copper IUD include:
Anemia
Backache
Painful or heavier menstruation
Pain with sex
Irregular periods
Vaginitis
Risks
There are a few rare risks to know about with IUDs:
Ectopic pregnancy: Getting pregnant with an IUD isn’t likely. But, if it happens, the pregnancy is more likely to be ectopic. This means the fertilized egg grows somewhere other than the uterus, usually in the fallopian tube, and it’s a surgical emergency.
Expulsion: This is when the IUD makes its way out of the uterus. The risk is less than 2% if it’s placed 4 or more weeks after giving birth. But the risk increases for IUDs placed closer to birth, especially vaginal birth. An expulsion might not cause symptoms, or it could result in cramps, pain with sex, or irregular bleeding.
Perforation: This is when the IUD punctures the wall of the uterus. It’s very rare. Many times there are no symptoms with perforation. Other times, it may cause pelvic or abdominal pain and abnormal bleeding. Depending on where it is, it may need to be surgically removed.
The risks of expulsion and perforation are why it’s important to check for your strings regularly. If you can’t find them, or if you have any symptoms out of the ordinary, contact your healthcare team to have a second look.
You shouldn’t get either IUD if you are pregnant or have:
An STI
Pelvic inflammatory disease
Cervical or endometrial cancer
Unexplained vaginal bleeding
You shouldn’t get the hormone-releasing IUD if you have breast cancer (current or past) or liver disease.
3. Depo-Provera injection
Depot medroxyprogesterone acetate (DMPA) is a progestin-only contraception. It’s given by injection every 3 months (4 times per year). The brand name is Depo-Provera, and it’s sometimes known as the “Depo shot” or the “birth control shot.” A healthcare professional can give you the shot, or you can self-administer it at home.
It prevents pregnancy by thickening the cervical mucus and preventing ovulation.
Benefits
Possible benefits of DMPA include:
Help with endometriosis pain
Lower risk of endometrial cancer
Safe to use right after giving birth
Safe to use while breastfeeding
Side effects
The most common side effect is irregular bleeding. Other side effects include:
Breast tenderness
Pain, bruising, or skin changes at the injection site
Risks
Using hormonal contraceptives increases the risk for blood clots (see below). DMPA has been linked to lower bone mineral density. Experts aren’t sure if this leads to a higher risk of fractures. This change in bone density is reversible after the injections are stopped. But it should still factor into your birth control decision.
You shouldn’t get DMPA if you are pregnant or have:
Breast cancer (current or recent)
Diabetes with complications
Heart disease
Liver disease
Lupus
History of stroke
Unexplained vaginal bleeding
4. Patch
The patch (Xulane, Twirla) contains estrogen and progestin, which are released through the skin into the body. It prevents pregnancy by inhibiting ovulation, thickening the cervical mucus, and thinning the uterus lining. But the combination of the two hormones is more effective at preventing ovulation than progestin-only formulations.
You apply 1 patch to your body once a week for 3 weeks, making sure to remove the old patch before applying a new one. It’s a good idea to change the spot where you apply the patch to prevent skin irritation from the adhesive on the patch. On week 4 of your cycle, don’t apply a new patch. You’ll get your period during this off week.
Benefits
Hormonal contraceptives like the patch can help symptoms related to periods or endometriosis. They can also make your periods lighter.
Side effects
Possible side effects include:
Headache
Skin irritation
Breast tenderness
Nausea
Spotting
Studies suggest that people who use the patch may be more likely to stop using it due to side effects than people who use the pill.
Risks
Using hormonal contraceptives increases the risk for blood clots (see below). Some evidence suggests that patches don’t work as well at protecting against pregnancy in women with high body fat.
Don’t use the patch for at least a few weeks after giving birth or if you are currently pregnant. Also avoid the patch if you have any of the following:
Blood clots (current or past)
Body mass index (BMI) of 30 or greater
Breast cancer (current or past)
Diabetes with complications
Gallbladder disease
Heart disease
High blood pressure that isn’t well managed with treatment
Liver disease
Certain people with lupus
Migraine with aura
Stroke
If you are older than 35 years and have the following, don’t use the patch:
Smoking
Diabetes with or without complications
Migraines
5. Ring
Contraceptive rings (NuvaRing and Annovera) are flexible rings that contain estrogen and progestin. The different brands work similarly.
You insert the ring into your vagina, where it releases hormones. It stays in place for 21 days at a time. You don’t need to remove it for sex. After 21 days, you remove the ring for 1 week, during which time you will most likely have a period. Then you either insert a new ring (if you’re using NuvaRing) or reinsert the same ring after cleaning it (if you’re using Annovera). An Annovera ring provides enough hormonal medication for 13 menstrual cycles (about 1 year).
Benefits
Benefits of the ring are similar to those of the patch.
Side effects
Possible side effects include the usual ones, like headache and breast tenderness. But the ring may also cause vaginal irritation and discharge. Studies suggest that people who use the ring might have fewer side effects and thus be less likely to stop using it than people who use the pill.
Risks
See below for more information on the risk of blood clots with hormonal contraceptives.
Don’t use the ring for at least a few weeks after giving birth or if you are currently pregnant. Avoid using the ring if you have any of the following:
Blood clots (current or past)
Breast cancer (current or past)
Diabetes with complications
Gallbladder disease
Heart disease
High blood pressure that isn’t well managed
Liver disease
Certain people with lupus
Migraine with aura
Stroke
If you are older than 35 years and have the following, don’t use the patch:
Smoking
Diabetes with or without complications
Migraines
6. FemCap and diaphragm
The cervical cap (FemCap) and diaphragm are reusable pieces of silicone that you insert into your vagina to cover your cervix before you have sex. These are known as “barrier methods” because they serve as a physical barrier that prevents sperm from reaching the uterus. They should be used with spermicide, which slows down sperm and makes it harder for them to reach an egg.
They don’t contain hormones, but they both require a prescription. Cervical caps are smaller in size than diaphragms and can be left in place longer.
Like most contraceptives, the cervical cap and diaphragm work best when they’re used correctly. For barrier methods, that means using them every single time before sex. Keep in mind that they need to be left in place for at least 6 hours after sex. They can be hard to use correctly, especially at first, and they’re more effective for people who have never given birth.
Benefits
Barrier methods are convenient in that you can carry them with you. They’re also an option for people looking for a nonhormonal contraceptive option.
Side effects
Spermicide is the most likely culprit of side effects. It can contribute to vaginal irritation and even allergic reactions. Spermicide may also increase the risk of urinary tract infections (UTI) and HIV infection.
Risks
If your body changes, like experiencing weight changes or after having a baby, you’ll probably need a new size of cervical cap or diaphragm. There’s a small risk of toxic shock syndrome with caps and diaphragms, so don’t leave one in for more than 24 hours. And don’t use it while you have your period.
7. Phexxi gel
Phexxi is the first contraceptive gel of its kind. The FDA approved it in mid-2020. It contains lactic acid, citric acid, and potassium bitartrate. It works by keeping the pH in the vagina low enough so sperm can’t move well. It doesn’t contain hormones or spermicide.
You need a prescription to get it, and it comes in a prefilled applicator, sort of like a tampon. It’s meant to be applied to the vagina within 1 hour before each sexual encounter.
Benefits
Possible benefits of Phexxi include:
Easy to use
Doesn’t contain any hormones
Can be used with other types of contraception, except the ring
Side effects
Phexxi gel may feel messy, although it’s meant to be less messy than traditional spermicide. Side effects reported with Phexxi use include:
UTI
Yeast infection
Burning, itching, and pain of the vulva and vagina
Risks
Very rarely, women using Phexxi experience serious UTIs or kidney infections. You also have to remember to use it in order for it to be effective.
Take our quiz: Types of birth control
How to choose the best birth control option for you?
With all of these options for contraception (and more over-the-counter (OTC) options), it might be hard to know how to choose. First, speak to your healthcare professional about your options. They can help you narrow it down based on whether you have any medical conditions to consider or if you take any medications.
Then, think about things like convenience, affordability, and efficacy. As you choose your birth control method, consider what’s most important to you:
Lifestyle: Are you OK with remembering to replace a patch or ring? Or would you rather use a form of birth control that lasts longer?
Hormones: Are you sensitive to hormones, or do you want to avoid them? Or are you looking for a hormonal birth control that will help with painful periods?
Affordability: Do you have insurance or want to avoid a large upfront cost?
Which forms of birth control are covered by insurance?
Keep in mind that the Affordable Care Act (ACA) says that healthcare plans must cover contraception prescribed by a healthcare professional. This includes all FDA-approved options, including the ones mentioned here. If you have coverage, and your healthcare team prescribes birth control, you shouldn’t be charged for the contraception or for a copay.
Note that employers may opt out of this policy if they have a “religious or moral objection” to providing coverage for contraception to their employees. Be sure to check your plan for more information.
How to save on nonpill birth control
If you are uninsured, underinsured, or want to go outside your insurance plan, alternative forms of birth control can still be an option. Here are some ways to save on nonpill birth control:
Save with GoodRx: GoodRx can help you save a significant amount off the retail price of many of these options, and it’s easy to use. Just search GoodRx to find coupons for the lowest prices near you.
Save with copay savings cards: Many manufacturers offer copay cards to help reduce the cost of medications. Usually, you must have commercial insurance to be eligible for these. For example, you may be able to get Annovera for as little as $0 using a savings card from the manufacturer. Check the GoodRx page for your birth control or visit the manufacturer’s website to see if this option is available.
Save with patient assistance programs: Many manufacturers offer their medications at reduced cost through patient assistance programs. For example, Bayer offers assistance for their IUD Mirena for qualifying individuals. Visit the manufacturer’s website or ask your healthcare team to see what options are available.
Visit a free clinic: Clinics like Planned Parenthood or ones that participate in the federal 340B program may offer alternatives to oral birth control at a reduced cost. You can also search for a Title X family planning clinic near you.
A note on birth control risks
Last but not least, it’s important to know that there are some medical risks linked to the use of hormonal contraceptives — not just the pill.
Risk of blood clots
Some types of hormonal birth control (including the ring, patch, and injection) increase the risk of blood clots. The risk is higher if you’re older than 40 years, smoke, or have certain medical conditions.
Risk of breast cancer
Use of hormonal birth control has been linked with a slightly higher risk of breast and cervical cancer. The risk is very small, and it likely goes away after birth control use is stopped. The exceptions are implants and injections, which don’t appear to increase the risk of breast cancer at this time.
It’s also important to note that hormonal birth control lowers your risk of other cancers, such as endometrial, ovarian, and colorectal cancers.
When choosing a form of contraception, it’s best to weigh all the pros and cons — not just these risks — to choose what’s best for you.
Frequently asked questions
Many people find long-acting methods like IUDs and implants to be convenient, because you can forget about them once they’re in place. Others may prefer the convenience of never having to worry about contraception again with surgical sterilization, but it’s permanent. It’s really a matter of personal preference.
Most types of birth control — except the Depo-Provera injection (DMPA) — actually don’t cause weight gain. Experts believe that any weight gain reported with birth control is due to water retention (more likely with hormonal contraception) or natural weight gain with age. Studies suggest even nonhormonal contraception like the copper IUD is linked with some change in weight.
If you’re looking for birth control without hormones, you have plenty of options. As mentioned above, barrier methods like the cervical cap, diaphragm, and condoms don’t have hormones. Lifestyle methods like withdrawal and natural family planning are also hormone-free, although they are less effective at preventing pregnancy. The copper IUDs are effective longer-term options, and surgical sterilization (tubal surgery or vasectomy) is often permanent.
Many people find long-acting methods like IUDs and implants to be convenient, because you can forget about them once they’re in place. Others may prefer the convenience of never having to worry about contraception again with surgical sterilization, but it’s permanent. It’s really a matter of personal preference.
Most types of birth control — except the Depo-Provera injection (DMPA) — actually don’t cause weight gain. Experts believe that any weight gain reported with birth control is due to water retention (more likely with hormonal contraception) or natural weight gain with age. Studies suggest even nonhormonal contraception like the copper IUD is linked with some change in weight.
If you’re looking for birth control without hormones, you have plenty of options. As mentioned above, barrier methods like the cervical cap, diaphragm, and condoms don’t have hormones. Lifestyle methods like withdrawal and natural family planning are also hormone-free, although they are less effective at preventing pregnancy. The copper IUDs are effective longer-term options, and surgical sterilization (tubal surgery or vasectomy) is often permanent.
The bottom line
If you’re interested in an effective alternative birth control that isn’t the pill, you have plenty of options. Selecting the best one for you is a personal choice, and what’s important to you may change at different points of your life. When choosing a birth control method, think about convenience, cost, and lifestyle. And consider if you want to address certain symptoms, like painful periods. Your healthcare team can help you figure out the best option that fits your unique needs.

Why trust our experts?




References
American Cancer Society. (2025). Endometrial cancer risk factors.
American College of Obstetricians and Gynecologists. (2014). Depot medroxyprogesterone acetate and bone effects.
American College of Obstetricians and Gynecologists. (2017). Long-acting reversible contraception implants and intrauterine devices.
American College of Obstetricians and Gynecologists. (2024). Hormonal contraception and risk of breast cancer.
American College of Obstetricians and Gynecologists. (2025). Long-acting reversible contraception (LARC): Intrauterine device (IUD) and implant.
American College of Obstetricians and Gynecologists. (2024). Progestin-only hormonal birth control: Pill and injection.
American College of Obstetricians and Gynecologists. (2025). Barrier methods of birth control: Spermicide, condom, diaphragm, and cervical cap.
Carvalho, N., et al. (2018). Control of endometriosis-associated pain with etonogestrel-releasing contraceptive implant and 52-mg levonorgestrel-releasing intrauterine system: Randomized clinical trial. Fertility and Sterility.
Centers for Disease Control and Prevention. (2024). Appendix B: Classifications for intrauterine devices.
Centers for Disease Control and Prevention. (2024). Appendix C: Classifications for progestin-only contraceptives.
Centers for Disease Control and Prevention. (2024). Appendix D: Classifications for combined hormonal contraceptives.
Centers for Disease Control and Prevention. (2024). Progestin-only pills.
Curtis, K. M., et al. (2017). Long-acting reversible contraception. New England Journal of Medicine.
Daniels, K., et al. (2025). Current contraceptive status among women aged 15-49: United States, 2022-2023. Centers for Disease Control and Prevention.
Evofem. (2023). Phexxi- lactic acid, l-, citric acid monohydrate, and potassium bitartrate gel [package insert]. DailyMed.
Faculty of Sexual & Reproductive Healthcare. (2019). FSRH CEU statement: Contraception and weight gain.
Fitzpatrick, D., et al. (2023). Combined and progestagen-only hormonal contraceptives and breast cancer risk: A UK nested case–control study and meta-analysis. PLoS Medicine.
Healthcare.gov. (n.d.). Health benefits & coverage.
Health Resources and Services Administration. (2025). 340B drug pricing program.
Lopez, L. M., et al. (2013). Skin patch and vaginal ring versus combined oral contraceptives for contraception. Cochrane Library of Systematic Reviews.
National Health Service. (2024). Side effects and risks of the diaphragm or cap.
Phexxi. (n.d.). Dosing & prescribing.
Planned Parenthood. (n.d.). How effective are cervical caps?
Planned Parenthood. (n.d.). Spermicide & contraceptive gel.
Samson, M., et al. (2015). Progestin and breast cancer risk: A systematic review. Breast Cancer Research and Treatment.
Serfaty, D. (2019). Update on the contraceptive contraindications. Journal of Gynecology Obstetrics and Human Reproduction.
Simmons, K. B., et al. (2016). Hormonal contraception and obesity. Fertility and Sterility.
Trimmier, M., et al. (2023). Does long-term use of depot medroxyprogesterone acetate increase the risk of osteoporosis? Evidence-Based Practice.
U.S. Food and Drug Administration. (2024). Birth control guide (chart).
World Health Organization. (2002). Nonoxynol-9 ineffective in preventing HIV infection.