Key takeaways:
Statins are a group of medications that treat high cholesterol levels. Names of statins include atorvastatin (Lipitor, Atorvaliq), rosuvastatin (Crestor), and simvastatin (Zocor, FloLipid).
There isn’t one best statin to take. No individual statin has been proved to be best at preventing heart attacks and strokes. But there is evidence that rosuvastatin and atorvastatin decrease harmful cholesterol more than other statins.
Some people will clearly benefit from taking a statin. But statins are not a good idea for others, based on individual risk factors. Work with your healthcare team to find out if statins are a good choice for you.
Save on related medications
Your body needs cholesterol to make cells, some hormones, and vitamin D. But too much cholesterol leads to atherosclerosis, which is the medical term for the buildup of sludge (also known as plaque) in your arteries.
Why does this matter? Arteries are the blood vessels that supply nutrients and oxygen to your body. When they get clogged, it reduces blood flow to tissues and organs. This prevents the delivery of vital nutrients and oxygen and can lead to a heart attack or stroke.
High cholesterol can be managed with dietary and lifestyle changes and by taking prescription medications such as statins. Below are details about what statins are used for and who should take them.
What are statins, and what are they used for?
Statins are a group of medications that lower cholesterol levels. They also help reduce the risk of heart attack and stroke.
Statins work by blocking an enzyme (protein) that your body uses to make cholesterol. By blocking this protein (called HMG-CoA reductase), statins lower the amount of cholesterol your body makes. This lowers your risk of developing atherosclerosis and atherosclerotic cardiovascular disease (ASCVD). ASCVD is a type of heart disease caused by atherosclerosis that can lead to heart attacks and stroke.
Statins have different effects on various cholesterol and cholesterol-related molecules:
Lowers LDL cholesterol levels: Low-density lipoprotein (LDL) is the “bad” type of cholesterol and is most closely linked to ASCVD. The lower the better.
Slightly raises HDL cholesterol: High-density lipoprotein (HDL) is the “good” type of cholesterol. The higher the better.
Lowers triglyceride levels: Triglycerides are a type of fat that your body makes from the foods you eat. High triglycerides are linked to a greater risk of heart disease. The lower the better.
Lowering LDL is the main way that statins lower the risk of cardiovascular disease. But statins may also lower levels of inflammatory proteins that contribute to cardiovascular disease.
What is high cholesterol?
When you have high cholesterol, it raises your risk of ASCVD and other health problems. If you have ASCVD, your coronary arteries, which bring oxygen to the heart, may be blocked. This can lead to heart attacks, heart failure, and chest pain (angina). And if the arteries in the neck (carotid arteries) are blocked, it can cause a stroke or transient ischemic attack (ministroke).
High cholesterol can also cause atherosclerosis in other parts of the body, including the legs, kidneys, and aorta (the largest artery in the abdomen). These types of atherosclerosis can cause pain, kidney problems, and even internal bleeding.
What side effects do statins cause?
Most people who take statins experience mild (or even no) side effects. But it’s good to know what could happen, including both common and rare but serious statin side effects.
Common or mild side effects reported by people taking statins include:
Headache
Fatigue
Nausea
Vomiting
Diarrhea
Rare but serious statin side effects include:
Rhabdomyolysis (muscle breakdown)
Kidney damage (typically happens only if a person experiences rhabdomyolysis)
Liver damage
Raised blood glucose (sugar), which can lead to Type 2 diabetes
There’s also a possible link between statins and memory loss. But research is unclear about whether statins truly cause dementia. Some studies suggest these cholesterol medications may contribute to it. Others have found that statins can actually help protect against dementia.
What are the names of some statins?
Statins are some of the most commonly prescribed medications in the U.S. The names of statins include:
Atorvastatin (Lipitor, Atorvaliq)
Fluvastatin (Lescol XL)
Rosuvastatin (Crestor)
Simvastatin (Zocor, FloLipid)
Pitavastatin (Livalo)
Who should take a statin?
When deciding whether you need a statin, your prescriber will look at more than your LDL levels. There are other risk factors for cardiovascular disease to keep in mind.
According to the 2026 guidelines from the American College of Cardiology and American Heart Association, several groups of people should be taking a statin. Four of these groups are discussed below.
Even if you don’t fall into one of the categories discussed below, you may need a statin if you’re at high risk for ASCVD. Information such as your age, sex, and health habits can be used to estimate your risk of developing ASCVD. Existing medical conditions are also taken into consideration.
Talk with your healthcare team about your individual risk level. They can help you decide if a statin is necessary. Statins are more likely to help people with high risk than those with low risk.
Keep in mind: If you’re over age 79, it's not clear if you'll get the same benefits from taking a statin, partly because you may also be at higher risk for side effects.
1. People with existing ASCVD
This includes people who have a history of:
Angina (chest pain) due to plaque in the coronary arteries
Heart attack or other conditions related to coronary artery blockage
Stroke or ministroke
Aortic aneurysm (a bulge in the aorta)
Revascularization surgery (a procedure that restores blood flow to the heart or other arteries)
In this group of people, the goal of using statins is to prevent further problems.
2. People ages 40 to 75 with diabetes
Diabetes raises your risk of cardiovascular disease. If you have diabetes, it’s important to address risk factors for cardiovascular disease. This includes managing your blood sugar and blood pressure, quitting smoking, and lowering your cholesterol.
3. Anyone whose LDL is 190 mg/dL or higher
Regardless of your age, and even if you don’t have existing ASCVD or diabetes, a statin is recommended if your LDL is this high.
4. People with familial hypercholesterolemia
This inherited condition affects 1 in 250 people worldwide. It causes extremely high cholesterol levels, even in childhood. Without treatment, people with familial hypercholesterolemia are at a higher risk for cardiovascular events, such as a heart attack, earlier in life.
Which statin is best?
Unfortunately, there isn’t a clear answer to this question. It depends on how you define “best.” There’s no evidence to date that proves one statin is the “best” at preventing cardiovascular disease. In addition, statins are available in a wide range of doses. In general, higher doses will lower LDL cholesterol more than lower doses.
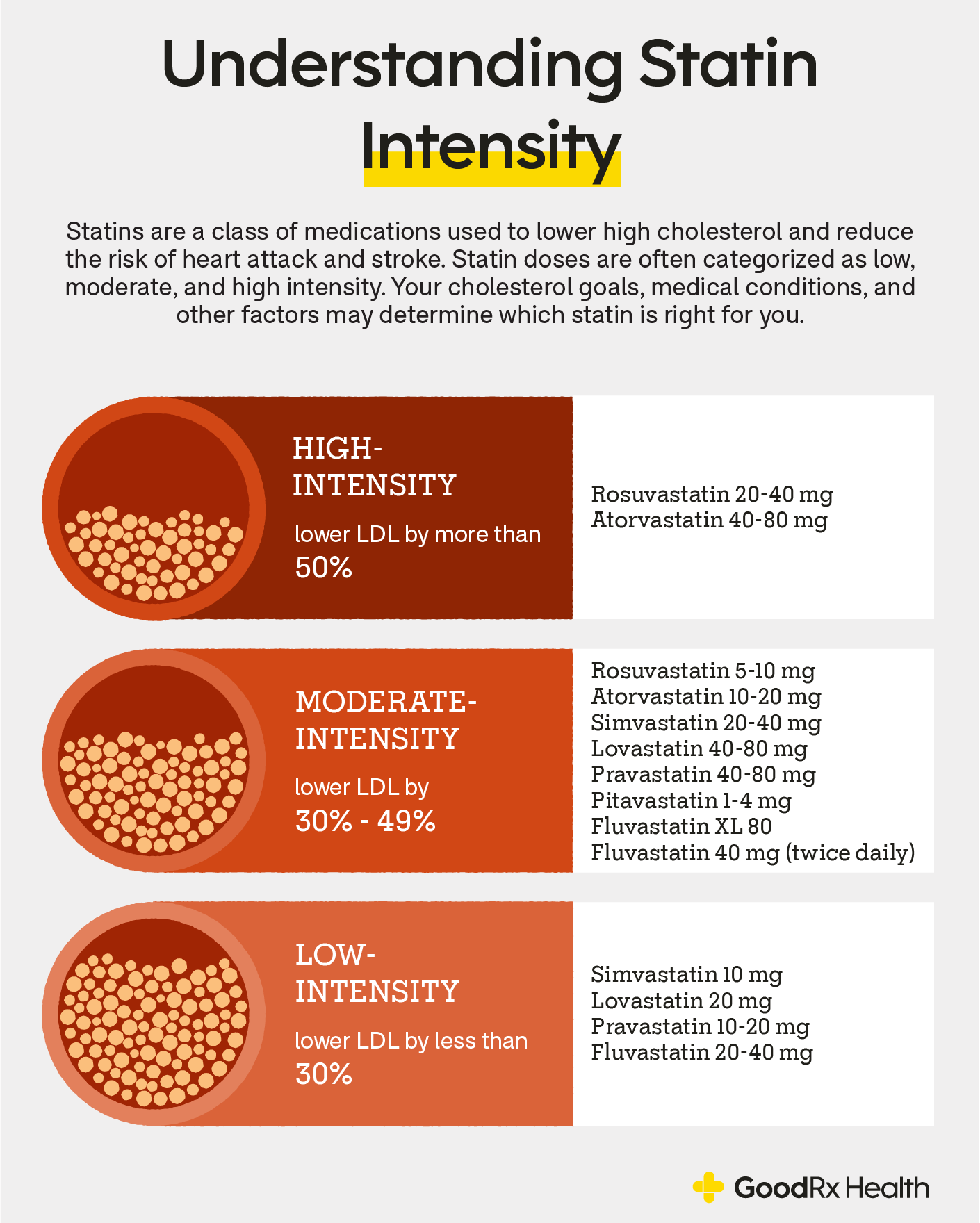
Still, some statins are more potent than others. This means that at equal doses, some statins will lower LDL more than others. Based on their potency and dose, statins can be categorized as high, moderate, and low intensity. You’ll notice that not all statins come in high-intensity doses, and some don’t come in low-intensity doses.
Rosuvastatin and atorvastatin may lower LDL cholesterol the most
Certain doses of rosuvastatin and atorvastatin reduce LDL more than other statins. Here’s the evidence backing this:
A 6-week clinical trial comparing rosuvastatin with atorvastatin, pravastatin, and simvastatin found that it lowered total cholesterol significantly more than the others and lowered triglycerides significantly more than simvastatin and pravastatin.
A 54-week clinical trial compared atorvastatin with fluvastatin, lovastatin, and simvastatin and found that atorvastatin was better at lowering LDL cholesterol than the other medications.
A systematic review of 75 clinical trials found that rosuvastatin and atorvastatin were the only statins that lowered LDL cholesterol by more than 40% (hence, they’re the only “high-intensity” statins).
Keep in mind: Rosuvastatin and atorvastatin lower LDL the most, but this doesn’t mean they’re the “best” at preventing ASCVD, including repeat heart attacks. To date, there has been no clinical trial that directly compares all of the available types of statins in a head-to-head fashion. But for some people who would benefit from significantly lowering LDL, rosuvastatin and atorvastatin may be a good option.
So, what’s the verdict?
The 2026 guidelines from the American College of Cardiology and American Heart Association don’t favor any specific type of statin over another. Instead, the guidelines recommend that people at very high risk for cardiovascular disease should take a high-intensity statin dose rather than a moderate- or low-intensity statin.
How should you take statins?
Your body makes most of its cholesterol at night. And some statins don’t stick around in the body very long. So it’s best to take these types of statins in the evening. Shorter-acting statins that you should take at night include:
Pravastatin
Lovastatin
Immediate-release forms of fluvastatin
You can take other statins at any time. Just be sure to take your dose about the same time each day. This helps the medication to work consistently.
Possible drug interactions
Statins interact with other medications, such as:
Fibrates, such as gemfibrozil (Lopid) and fenofibrate (Tricor)
Transplant medications, such as tacrolimus (Prograf)
Colchicine (Colcrys, Lodoco, Mitigare)
HIV medications, such as ritonavir (Norvir)
Paxlovid (nirmatrelvir / ritonavir)
Warfarin (Coumadin, Jantoven)
This isn’t a full list of all statin interactions. Share a list of medications and supplements you take with your prescriber and pharmacist. This list can help your healthcare team identify and manage potential interactions.
Can you have grapefruit juice when taking a statin?
Grapefruit interferes with how your body processes some statins. This can cause certain statins to hang around in your body at higher levels and for longer periods than usual. The statins affected by grapefruit include atorvastatin, simvastatin, and lovastatin. But the other types of statins, such as rosuvastatin, aren’t known to be affected.
The specific amount of grapefruit juice that's considered “risky” varies depending on the person and the situation. And experts don’t always agree on how much grapefruit juice is safe to have with statins. So talk to your prescriber and pharmacist before combining grapefruit juice with statins. They can help you decide how much, if any, is safe for you.
What about drinking alcohol?
It’s ideal to avoid alcohol while taking statins, especially if you also have liver problems. Alcohol raises the risk of certain statin side effects, such as liver damage. Drinking also raises your cholesterol. So your statin may not work as well with alcohol in the mix.
But if you don’t have liver disease, having an occasional drink is unlikely to cause serious harm. Ask your prescriber if this would be OK for you before drinking alcohol while taking statins.
Is it safe to stop taking your statin?
You shouldn’t stop taking a statin without talking to your prescriber. People sometimes want to stop taking statins because they:
Experience side effects
Worry about future side effects
Feel uncertain about the benefit
But the evidence is quite clear. Stopping a statin without a plan raises your risk of:
Higher LDL levels
New or worse blockages in your blood vessels
Hospital visits associated with a cardiovascular issue
Chest pain
Heart attack
Stroke
If you’re having trouble taking your statin regularly, talk to your healthcare team. Oftentimes, switching statins helps manage side effects. And if needed, there are alternative cholesterol medications that provide similar benefits.
How to save on statins
There are ways to save on your statin prescription. GoodRx can help you navigate your options, which may include GoodRx discounts, copay savings cards, and patient assistance programs.
For instance, anyone with a valid prescription, regardless of insurance status, can use GoodRx to purchase a 30-day supply of brand-name Lipitor at an exclusive cash price.
You can find statin prices as low as about $12 with a free GoodRx discount.
Frequently asked questions
Statins interact with several medications and substances, including:
Alcohol
Grapefruit
Fibrates, such as gemfibrozil (Lopid) and fenofibrate (Tricor)
Transplant medications, such as tacrolimus (Prograf)
Colchicine (Colcrys, Lodoco, Mitigare)
HIV medications, such as ritonavir (Norvir)
Paxlovid (nirmatrelvir / ritonavir)
Warfarin (Coumadin, Jantoven)
In some cases, you may need to avoid combining statins with these medications and substances. Other times, interactions can be managed by adjusting doses or limiting grapefruit or alcohol. Discuss statin interactions with your prescriber and pharmacist.
If you take statins, your LDL and triglyceride levels should go down. Your HDL may also go up slightly. These changes to your cholesterol levels can help lower your risk of serious cardiovascular events, such as heart attack and stroke.
Some people taking statins report mild side effects, such as muscle pain, fatigue, or headache. Very rarely, statins can cause serious side effects, such as muscle breakdown or liver damage. Discuss your risk for statin side effects with your prescriber. For most people, the benefits of statins greatly outweigh the potential risks.
It’s unclear whether statins cause dementia. Some studies show a link between statins and memory issues. Other studies suggest that statins protect against developing dementia. Discuss your personal risks with your prescriber.
Statins interact with several medications and substances, including:
Alcohol
Grapefruit
Fibrates, such as gemfibrozil (Lopid) and fenofibrate (Tricor)
Transplant medications, such as tacrolimus (Prograf)
Colchicine (Colcrys, Lodoco, Mitigare)
HIV medications, such as ritonavir (Norvir)
Paxlovid (nirmatrelvir / ritonavir)
Warfarin (Coumadin, Jantoven)
In some cases, you may need to avoid combining statins with these medications and substances. Other times, interactions can be managed by adjusting doses or limiting grapefruit or alcohol. Discuss statin interactions with your prescriber and pharmacist.
If you take statins, your LDL and triglyceride levels should go down. Your HDL may also go up slightly. These changes to your cholesterol levels can help lower your risk of serious cardiovascular events, such as heart attack and stroke.
Some people taking statins report mild side effects, such as muscle pain, fatigue, or headache. Very rarely, statins can cause serious side effects, such as muscle breakdown or liver damage. Discuss your risk for statin side effects with your prescriber. For most people, the benefits of statins greatly outweigh the potential risks.
It’s unclear whether statins cause dementia. Some studies show a link between statins and memory issues. Other studies suggest that statins protect against developing dementia. Discuss your personal risks with your prescriber.
The bottom line
High cholesterol levels often require treatment with prescription medications called statins. Statins are known to lower the risk of cardiovascular disease in people who need them. This means decreasing the risk of major health issues such as heart attack and stroke.
The names of different statins include rosuvastatin (Crestor), atorvastatin (Lipitor, Atrovaliq), and simvastatin (Zocor, FloLipid). Currently, there’s not one type of statin that’s considered “best” at preventing heart attacks or strokes. But certain doses of rosuvastatin and atorvastatin are known to lower LDL cholesterol more than other types of statins.
Certain groups of people clearly benefit from statins. This includes people who have existing cardiovascular disease, LDL levels of 190 mg/dL or higher, or diabetes (and are between the ages of 40 and 75). But other people may also benefit from statins, depending on their risk factors for cardiovascular disease. If you’re wondering whether you need a statin, talk to your healthcare provider about the possible risks and benefits.

Why trust our experts?




References
American Heart Association. (n.d.). The American Heart Association PREVENT online calculator.
Blumenthal, R. S., et al. (2026). 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation.
Brown, A. S., et al. (1999). Treating patients with documented atherosclerosis to national cholesterol education program-recommended low-density-lipoprotein cholesterol goals with atorvastatin, fluvastatin, lovastatin and simvastatin. Journal of the American College of Cardiology.
ClinCalc. (2025). ClinCalc DrugStats database. Agency for Healthcare Research and Quality.
Family Heart Foundation. (n.d.). Familial hypercholesterolemia.
He, W. B., et al. (2023). The effects of statins on cardiovascular and inflammatory biomarkers in primary prevention: A systematic review and meta-analysis. Heart, Lung and Circulation.
Jones, P. H., et al. (2003). Comparison of the efficacy and safety of rosuvastatin versus atorvastatin, simvastatin, and pravastatin across doses (STELLAR* trial). The American Journal of Cardiology.
Naci, H., et al. (2013). Comparative benefits of statins in the primary and secondary prevention of major coronary events and all-cause mortality: A network meta-analysis of placebo-controlled and active-comparator trials. European Journal of Preventive Cardiology.
National Heart, Lung, and Blood Institute. (2024). What is atherosclerosis? National Institutes of Health.
Peixoto, C., et al. (2024). Discontinuation versus continuation of statins: A systematic review. Journal of the American Geriatrics Society.
Weng, T.-C., et al. (2010). A systematic review and meta-analysis on the therapeutic equivalence of statins. Journal of Clinical Pharmacy and Therapeutics.
Zhou, Z., et al. (2005). Effectiveness of statins for secondary prevention in elderly patients after acute myocardial infarction: An evaluation of class effect. Canadian Medical Association Journal.
Zhou, Z., et al. (2006). Are statins created equal? Evidence from randomized trials of pravastatin, simvastatin, and atorvastatin for cardiovascular disease prevention. American Heart Journal.