

Key takeaways:
Autoimmune diseases commonly show up on the skin in the form of rashes. Skin changes and rashes may be the first sign of an underlying autoimmune disease.
These skin changes can include scaly patches, open sores, or blisters. Rashes may also show up on various parts of the body.
Treatment for autoimmune skin conditions also involves treating the underlying condition. Sun protection is also key for many of these conditions.
The skin is the largest organ in your body, and it can tell you a lot about your health. In fact, your skin is an important part of your immune system. Many autoimmune conditions can affect your skin and cause rashes. In fact, these skin changes may be the first — or only — symptom.
Let’s take a closer look at autoimmune rashes (with pictures), what causes them, and the best treatment options.
What causes an autoimmune rash?
When you have an autoimmune condition, your immune system mistakenly attacks normal parts of your body — and your skin can be a target for that attack. Some autoimmune conditions, like alopecia areata, only affect your skin. Others, like rheumatoid arthritis, can affect your skin as part of a multisystem disorder. A multisystem disorder is one that affects many parts of the body.
Because your skin is so visible, a rash may be the first sign of an underlying autoimmune disorder.
What does an autoimmune rash look like?
What an autoimmune rash looks like will vary, since different autoimmune conditions cause different skin changes and symptoms. Some symptoms are common, like itchy skin or changes in skin color. Other symptoms may be more specific to the underlying condition.
Here are some images of common autoimmune rashes.
1. Pink, red, violet, or brown rashes
On darker skin, rashes can look more violet or brown. On lighter skin, they tend to be pink or red.

2. Scaly patches
Scaly areas can be white or gray and range from patchy to pretty thick.

3. Open sores
Open sores can happen on your skin, and they’re also common inside your mouth or on your genitals.

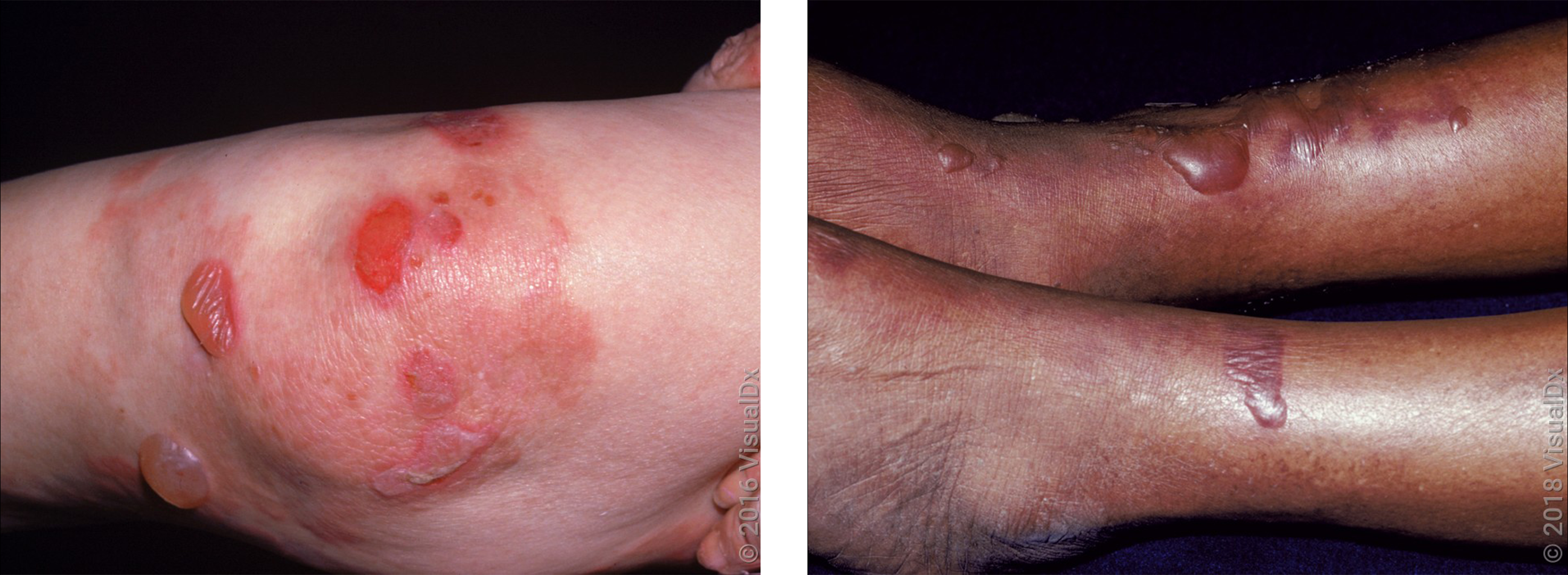
4. Blisters
Blisters can be small or large. Depending on the cause, they can be firm to the touch or they could break easily.

5. Crusty skin
Crusty patches often appear alongside rashes, blisters, or open sores.

Next, we’ll discuss common skin changes seen in certain autoimmune diseases.
Read more like this
Explore these related articles, suggested for readers like you.



Autoimmune rashes on the face
Two autoimmune diseases — lupus and dermatomyositis — cause rashes that can affect the face in different ways.
Lupus
Lupus is a chronic autoimmune disease that most commonly affects women ages 15 to 44. There are a few different types of lupus, including systemic lupus and cutaneous lupus.
Systemic lupus affects many organs and structures, in addition to the skin, including your:
Kidneys
Joints
Heart
Blood vessels
The first sign of systemic lupus is a butterfly rash on your face. This pink-red or violet-brown rash gets its name from its butterfly shape across the cheeks and bridge of your nose. In some people, it can itch or hurt, and it’s often mistaken for sunburn.

Cutaneous lupus is another form of lupus that mainly affects your skin. The two main types of cutaneous lupus cause different types of rash:
Subacute cutaneous lupus: This causes round, scaly patches on skin that’s exposed to the sun. These patches can be red, violet, or brown.
Discoid lupus: This causes thick, discolored, and scaly patches on your face, scalp, or ears. These patches may be associated with hair loss and be brown, pink, or white.
If you have lupus that affects your skin, your care team may order more tests, like blood work. This is to make sure you don’t have systemic lupus.
Dermatomyositis
Dermatomyositis is a rare autoimmune disease that causes muscle weakness and skin changes. It can sometimes cause difficulty breathing or a cough. It usually affects children between the ages of 5 and 15 and adults between the ages of 40 and 60.
One early sign of dermatomyositis is a heliotrope face rash. This is a reddish-purple to brown-violet rash on your eyelids.

Dermatomyositis can also cause skin changes on other parts of your body, including:
Red, pink, or purple bumps on the outer joints of your hand, knees, or elbows
Red, purple, brown, or discolored skin on sun-exposed areas, including your chest, shoulders, neck, and upper back
There’s no cure for lupus or dermatomyositis. But medications that lower your immune response can help manage symptoms.
Blisters in the skin
Many autoimmune diseases cause skin blisters. Blisters can look different depending on which part of your skin is involved and which the underlying autoimmune condition you have. Some blisters are large, firm, and full of fluid. Others can be small and form yellow crusts.
Dermatitis herpetiformis
Dermatitis herpetiformis is a chronic autoimmune skin condition linked to celiac disease. It occurs as a reaction to eating gluten, a protein that’s in many foods, like wheat and rye.
Between 10% to 15% of people with celiac disease get a dermatitis herpetiformis skin rash. This rash usually begins between the ages of 30 to 40 and appears as extremely itchy blisters, along with red to violet bumps and sores. It’s most commonly found on the:
Scalp
Elbows
Knees
Buttocks

Many people also experience:
Stomach pain
Cramping
Diarrhea
For some people, symptoms come and go, which makes it harder to diagnose.
Treatment includes removing all gluten from your diet. Some medications can also help. (More about treatments below.)
Pemphigoid
Pemphigoid is a group of rare autoimmune diseases that form blisters in your skin. The most common type is called bullous pemphigoid. It usually affects people over the age of 70.
Bullous pemphigoid can cause itchy, firm blisters on any part of your skin, including your mouth and genitals. Some people will have just a few spots, but for others it can cover large parts of the body.
Neurologic diseases — like dementia and Parkinson’s disease — are more common in people with bullous pemphigoid.
There are different medications that can help treat pemphigoid. For many people, the rash will go away on its own after a few years.
Pemphigus
Pemphigus is another group of rare autoimmune diseases that form blisters in the skin. But it’s quite different from pemphigoid. Pemphigus vulgaris is the most common type, and it usually affects middle-aged and older adults.
This causes painful ulcers and sores that can join together. Most people get small blisters that are red, violet, or brown. These blisters break easily but don’t itch. Often, the blisters start in the mouth and then spread to other parts of the skin. Some people will have only a few blisters. Others will have large areas of their skin involved.
In people with darker skin, pemphigus can leave light or dark patches, called post-inflammatory hypopigmentation and hyperpigmentation, that can take months to fade.


People with pemphigus might also get skin infections where there are blisters. In some cases, pemphigus vulgaris can become life threatening, if it’s not treated.
Although there’s no cure for pemphigus, there are good treatments that can control symptoms.
Thick or hardened skin
Some autoimmune rashes, like psoriasis and scleroderma, can cause a change in your skin’s thickness or texture. In some situations, they can also affect other parts of your body.
Psoriasis
Psoriasis is a common autoimmune disease that affects about 3% of adults in the U.S. It’s a chronic condition that causes patches of skin to grow too quickly.
There are different types of psoriasis, but plaque psoriasis is the most common. In lighter skin tones, this causes red patches with thick, white scales. In darker skin tones, the patches can be violet or brown with gray scales. These patches usually affect the:
Elbows
Knees
Lower back

Beyond the skin, people with psoriasis can also have other conditions, like:
Psoriatic arthritis, which causes painful, swollen joints
Psoriasis is usually a lifelong condition, and the best psoriasis treatment for you will depend on how severe your symptoms are. Treatment usually includes medicated creams, pills, or shots that can help lower your immune system’s response.
Scleroderma
Scleroderma is an autoimmune disease that causes your body to make too much collagen. Collagen is a protein found in your skin and other tissues. Although anyone can get scleroderma, it usually affects women between the ages of 30 and 50.
There are two main types:
Localized scleroderma: Also called morphea, this affects your skin and underlying tissue.
Systemic scleroderma: Also called systemic sclerosis, this can affect your skin and other organs, like your heart, lungs, kidneys, and blood vessels. This is the more serious type.
Both types of scleroderma cause patches of hardened, thick skin to form, which feels firm to the touch and can appear shiny. The patches are usually darker than normal skin and range from red to brown, or they can be lighter or white in color. They can be round or oval or form lines along your arms, legs, or forehead.

There’s no cure for scleroderma, but treatments can help manage the different symptoms. Some people with localized scleroderma might not need treatment, since skin changes might go away on their own.
Sores in the mouth or genitals
Mouth ulcers, like canker sores, are common and usually go away on their own. If mouth ulcers keep coming back, or if you also have them on the genitals, they could be a sign of a rare autoimmune disorder called Behçet disease.
Behçet disease can happen at any age, but symptoms usually begin in a person’s 20s and 30s. Experts don’t know the exact cause, but many symptoms result from inflammation of blood vessels. The condition can be different from person to person, and symptoms often come and go.
Some other symptoms include:
Skin rashes (acne-like spots, blisters, or painful, firm bumps)
Eye problems (like blurred vision, pain, or sensitivity to light)
Diarrhea
Headaches

There’s no cure for Behçet disease, but symptoms can usually be managed with medication. In some people, symptoms go away for a period of time (remission), and treatment may not be needed for a while.
Keep in mind that other autoimmune diseases, including lupus and pemphigus, can also cause sores in the mouth or genitals. If you have these symptoms, it’s a good idea to visit your primary care provider or dermatologist so they can help find the underlying cause.
How are autoimmune rashes diagnosed?
Diagnosing an autoimmune rash starts with a medical history and physical exam. Your dermatologist or another healthcare professional will ask about your symptoms and examine your rash. Depending on what they find, you may need additional tests, including:
A skin biopsy: This minor in-office procedure involves removing a small piece of skin tissue for analysis under a microscope.
Blood tests: These can check for inflammation or certain antibodies, like antinuclear antibodies (ANA).
Imaging tests: A CT scan or other imaging may be needed if an autoimmune disease is affecting internal organs.
Treating autoimmune skin rashes
The most important part of treating autoimmune rashes is treating the underlying condition.
Most medications work by lowering inflammation and suppressing your immune response. When only small areas of skin are affected, medicated creams or lotions may be enough. Pills or shots are more common when larger areas of skin or other organs are involved.
Here are some common medications used to treat autoimmune diseases:
Corticosteroids: These help block inflammation and can be used to treat most autoimmune diseases. Corticosteroids come as medicated creams, injections, or pills.
Methotrexate: This is a pill that helps to lower your immune system response. Methotrexate (Rheumatrex) is used to treat many autoimmune diseases, including lupus, dermatomyositis, psoriasis, pemphigus, and pemphigoid.
Hydroxychloroquine: Hydroxychloroquine (Plaquenil) is a pill that’s usually used to treat malaria, but it also works well for lupus.
Dapsone: Dapsone (Aczone) is a pill that’s usually used to treat certain infections, but it’s also effective for dermatitis herpetiformis.
Biologics: These are newer medications that block specific molecules in your immune system. Most biologics are given as shots. Etanercept (Enbrel) treats psoriasis or psoriatic arthritis. Rituximab (Rituxan) treats pemphigus vulgaris. Belimumab (Benlysta) treats systemic lupus.
Do any over-the-counter treatments work?
It depends. Some over-the-counter (OTC) products can help, but they may not be strong enough to use as the first treatment. In certain situations, products with these ingredients may help:
For mild rashes: Hydrocortisone is a low-strength steroid cream that may help with mild rashes that occur in autoimmune disease.
For psoriasis: Salicylic acid, urea, or coal tar can help treat psoriasis.
For itchy rashes: Calamine or menthol can help soothe some itchy rashes.
Using sun protection if you have an autoimmune condition
Sun protection is an important part of treatment for many autoimmune rashes, especially those caused by lupus and dermatomyositis. Even small amounts of sun exposure can worsen skin symptoms. So, wearing sunscreen with at least SPF 30 every day is important.
Psoriasis is one autoimmune condition where ultraviolet (UV) light is used as a treatment (phototherapy). Although natural sunlight may help with symptoms, it’s not always recommended.
If you have psoriasis, talk with your primary care provider or dermatologist about what’s right for you. Keep in mind that some medications used to treat autoimmune diseases can also make your skin more sensitive to the sun.
Frequently asked questions
No, there’s no proven way to reset your immune system. But practicing these healthy habits may help reduce flare-ups:
Prioritizing good sleep
Avoiding known triggers
Eating a whole-foods diet that’s low in sugar and low in ultra-processed foods
Many medications also work by calming an overactive immune system. Talk with your healthcare team about which approach makes sense for you.
Many people with Sjogren’s disease don’t develop a rash. This condition more commonly causes dry eyes and a dry mouth.
If skin symptoms do occur, they may include:
Vasculitis (blood vessel inflammation that causes multiple red or purple spots on the skin, often on the legs)
Decreased sweating
If you notice any skin changes along with symptoms of dry eyes or mouth, talk to a healthcare professional to see if Sjogren’s could be the cause.
No, there’s no proven way to reset your immune system. But practicing these healthy habits may help reduce flare-ups:
Prioritizing good sleep
Avoiding known triggers
Eating a whole-foods diet that’s low in sugar and low in ultra-processed foods
Many medications also work by calming an overactive immune system. Talk with your healthcare team about which approach makes sense for you.
Many people with Sjogren’s disease don’t develop a rash. This condition more commonly causes dry eyes and a dry mouth.
If skin symptoms do occur, they may include:
Vasculitis (blood vessel inflammation that causes multiple red or purple spots on the skin, often on the legs)
Decreased sweating
If you notice any skin changes along with symptoms of dry eyes or mouth, talk to a healthcare professional to see if Sjogren’s could be the cause.
The bottom line
Autoimmune diseases can show up in your skin as different types of rashes. These skin changes may be the first sign of an underlying condition. If you develop an unexplained rash, sores, or skin changes, it’s important to see your primary care provider or dermatologist. They can help you get a diagnosis and the right treatment.

Why trust our experts?



Images used with permission from VisualDx (www.visualdx.com).
References
American Academy of Allergy, Asthma and Immunology. (2024). Immunosuppressive medication for the treatment of autoimmune disease.
American Academy of Dermatology. (n.d.). Pemphigus: Diagnosis and treatment.
American Academy of Dermatology. (n.d.). Psoriasis: Overview.
American Academy of Dermatology. (n.d.). Scleroderma: Overview.
Barker, S., et al. (2021). Sjögren syndrome. DermNet.
Celiac Disease Foundation. (n.d.). Dermatitis herpetiformis.
Centers for Disease Control and Prevention. (2024). Lupus basics.
Chellet, R., et al. (2019). Autoimmune diseases in dermatology. DermNet.
Elmets, C. A., et al. (2019). Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with awareness and attention to comorbidities. Journal of the American Academy of Dermatology.
Genetic and Rare Diseases Information Center. (2025). Behcet disease. National Institutes of Health.
Genetic and Rare Diseases Information Center. (2025). Dermatomyositis. National Institutes of Health.
Genetic and Rare Diseases Information Center. (2025). Localized scleroderma. National Institutes of Health.
Genetic and Rare Diseases Information Center. (2025). Pemphigus vulgaris. National Institutes of Health.
Kridin, K., et al. (2018). The growing incidence of bullous pemphigoid: Overview and potential explanations. Frontiers in Medicine.
Ludmann, P. (2022). Lupus and your skin: Overview. American Academy of Dermatology.
Ludmann, P. (2022). Lupus and your skin: Self-care dermatologists recommend. American Academy of Dermatology.
Lupus Foundation of America. (2023). Lupus symptoms.
Lupus Foundation of America. (2024). What is systemic lupus erythematosus (SLE)?
MedlinePlus. (n.d.). Behçet disease.
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2023). Psoriasis. National Institutes of Health.
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2023). Scleroderma. National Institutes of Health.
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2024). Pemphigus. National Institutes of Health.
National Organization for Rare Disorders. (2018). Bullous pemphigoid.
National Organization for Rare Disorders. (2018). Dermatitis herpetiformis.
National Psoriasis Foundation. (2025). Phototherapy for psoriasis.
National Scleroderma Foundation. (n.d.). What is scleroderma?
Ngan, V., et al. (2025). Adult-onset dermatomyositis. DermNet.
Nyugen, A. V., et al. (2019). The dynamics of the skin’s immune system. International Journal of Molecular Sciences.
Stevens, N. E., et al. (2019). Skin barrier and autoimmunity — Mechanisms and novel therapeutic approaches for autoimmune blistering diseases of the skin. Frontiers in Medicine.
Vesely, M. D. (2020). Getting under the skin: Targeting cutaneous autoimmune disease. Yale Journal of Biology and Medicine.












