
Actinic Keratosis in Pictures: Early Signs You Shouldn’t Ignore


Key takeaways:
Actinic keratosis is a skin lesion caused by chronic sun damage. Having one or more increases your risk of developing skin cancer.
Actinic keratosis looks like a rough, scaly patch of skin. It usually develops on sun-exposed parts of your skin, like your face, scalp, or ears.
Effective treatments include surgical procedures, medicated creams, and photodynamic therapy.
Table of contents

If you have a scaly patch of skin on your face that doesn’t heal, it could be a sign of sun-damage called an actinic keratosis. These spots are very common, and they’re caused by chronic ultraviolet (UV) light from the sun and/or tanning beds.
Having an actinic keratosis increases your risk of developing skin cancer, so it’s important to know how to spot one and what to do about it. Here, we’ll review what an actinic keratosis looks like (with pictures) and the different treatment options available.
What is an actinic keratosis?
An actinic keratosis (also called solar keratosis) is a precancerous spot on the skin. This means that if it’s not treated, it could turn into a type of skin cancer called squamous cell carcinoma (SCC).
Only about 5% to 10% of actinic keratoses turn into skin cancer. But it’s impossible to predict which ones will and which won’t. To lower your risk of developing skin cancer, it’s important to learn how to identify actinic keratosis, and treat it.
Actinic keratosis symptoms
For many people, actinic keratosis doesn’t have any symptoms. But some people may experience:
Burning
Itching or tingling
Bleeding
Crusting
What does skin cancer look like? See pictures of different types of skin cancer, in different skin tones.
Black people can get skin cancer, too. But skin cancer can look different in darker skin tones, so it can be easier to miss. Learn what to look for, with pictures.
Living with skin cancer: One woman shares her story living with — and recovering from — stage 4 melanoma.
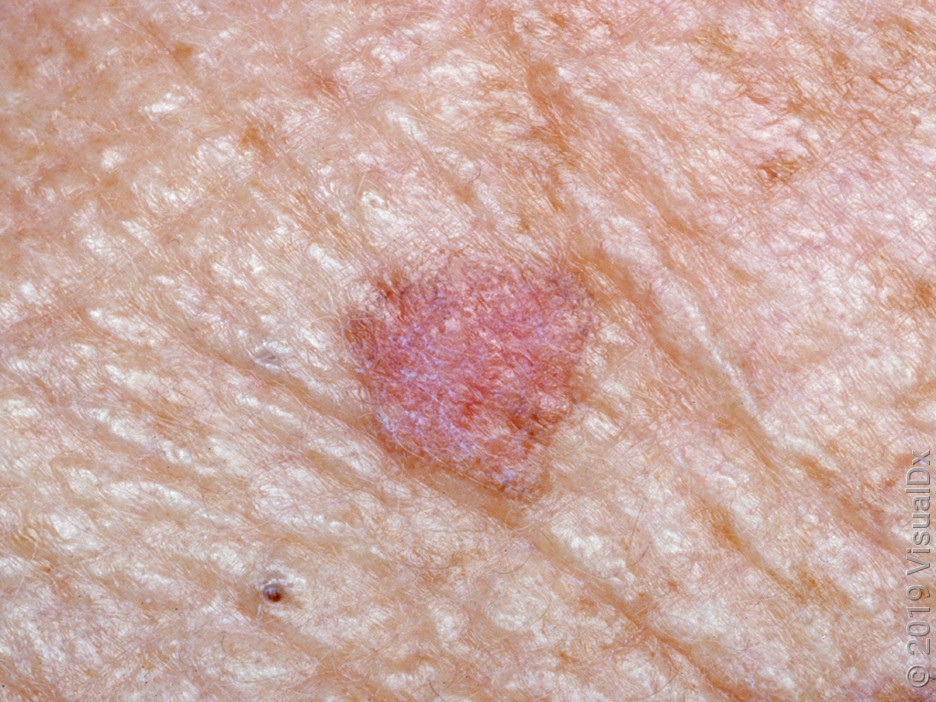
What does an actinic keratosis look like?
Actinic keratoses look like rough, scaly, or crusty patches of skin. It’s common to have more than one spot at a time.
These spots share certain characteristic features, such as:
They don’t go away.
They vary in size, but usually not bigger than a quarter.
They vary in color, from red or pink to white, tan, or brown.
Spots can be flat or raised.
They feel rough to the touch.
They commonly develop on sun-exposed parts of the body (face, scalp, ears, neck, arms, and the back of the hands).
Here are some pictures of actinic keratosis in different skin tones and on different parts of the body.





What is the difference between actinic keratosis and seborrheic keratosis?
A seborrheic keratosis is a type of skin growth that can look like an actinic keratosis — but isn’t. Unlike actinic keratosis, seborrheic keratosis is benign. That means that it will never turn into cancer.
It’s common to get one or more seborrheic keratoses as you get older. But if you have a new skin bump and you’re not sure what it is, it’s always best to get it checked out by your primary care provider, or a dermatologist.
A seborrheic keratosis usually doesn’t have any symptoms, but it can sometimes itch or hurt. Here are some ways they look different from actinic keratoses. A seborrheic keratosis is:
Usually tan, brown, or black in color
Raised and bumpy
Waxy or scaly in texture
Usually larger than actinic keratosis, typically bigger than a quarter
Here are some pictures of seborrheic keratoses.


Risk factors for actinic keratosis
Chronic sun exposure is the main risk factor for developing actinic keratosis. This is why they usually develop on sun-exposed skin in older people who’ve had decades of unprotected sun exposure.
Some other risk factors include:
Being male
Being older than 40 years
Having fair skin
Having a weakened immune system
Living near the equator (where UV rays are stronger)
Using tanning beds
Experiencing previous actinic keratoses or any type of skin cancer
Treatment for actinic keratosis
The goal of treatment for actinic keratosis is to help lower your risk of developing skin cancer, reduce any associated symptoms, and improve the cosmetic appearance of the skin.
Choosing the right treatment for you depends on a few different factors, including how many actinic keratosis spots you have, where they are, and your personal preferences:
For one or a few lesions, surgical treatments (like cryosurgery) are usually the easiest and most effective treatments.
For multiple spots, treatments that cover large areas of skin are better. These include topical creams, photodynamic therapy (PDT), and chemical peels.
It’s also common to combine different treatments for best results.
Surgical treatments
Surgical treatments are procedures done in the office. Recovery can range from a few days to weeks depending on the procedure used and the size of the area treated.
Cryosurgery: Liquid nitrogen is applied to freeze and destroy the cells.
Curettage and electrodessication: A blade is used to scrape and remove the lesion. If needed, heat is used to stop any bleeding.
Laser surgery: A laser beam (like a carbon dioxide laser) is used to destroy the damaged skin.
Chemical peel: A high-strength chemical peel, like trichloroacetic acid, is used to remove the damaged outer skin layers.
Topical treatments
Topical treatments are prescription creams and gels that are applied directly to the actinic keratosis spots. They work by stopping abnormal cell growth and destroying precancerous skin cells.
One advantage to topical treatments is that they can be applied at home. Depending on which cream you use, you’ll apply it once or twice daily for a set period of time (usually 2 to 4 weeks). These creams can cause skin irritation and crusting, and it can take several weeks for the skin to heal after treatment.
Topical treatments for actinic keratosis include:
5-fluorouracil (Efudex)
Imiquimod (Aldara)
Diclofenac (Solaraze)
Tirbanibulin (Klisyri)
Ingenol mebutate (Picato)
While all treatments are effective, some dermatology experts recommend 5-fluorouracil and imiquimod over the others. In practice, your dermatologist can help you find the best treatment for you.
Photodynamic therapy
Photodynamic therapy (PDT) uses a combination of a photosensitizing medication and light beam to treat actinic keratosis. It’s an in-office procedure. Here’s an overview of how it works:
Application: A photosensitizing medication is applied directly to the area, and it’s absorbed by the precancerous cells (this makes them very sensitive to light).
Incubation: The person waits for a preset amount of time, usually 60 to 90 minutes.
Exposure: The area is exposed to a specific wavelength of light (usually blue light), which destroys the precancerous cells but not healthy skin.
Treatment with PDT can cause mild tingling during treatment and then skin redness and swelling afterwards.
Sun protection
Studies show that using sunscreen to protect against ultraviolet exposure can lower the risk of developing actinic keratosis. When you already have actinic keratosis, this means you have sun-damaged skin. So, protection from further sun damage is a very important part of treatment.
Follow these tips for the best ways to protect your skin from sun damage:
Use broad-spectrum sunscreen of SPF 30 or higher.
Wear sun-protective clothing.
Try to avoid direct sun exposure during the hottest hours of the day, and stay in the shade as much as possible.
When to see a doctor
If you notice a new scaly patch that doesn’t go away within 2 weeks, or any new or changing skin spot, it’s best to be checked out by a trained healthcare professional. This could be your primary care provider or a dermatologist. They can look for actinic keratosis or skin cancer and recommend the next best steps to treat it.
Frequently asked questions
No. You can’t treat or remove an actinic keratosis at home on your own. But, some treatments prescribed by your healthcare team may be used at home.
Studies show that it takes about 2 years for an actinic keratosis to turn into skin cancer. Keep in mind that only about 10% of actinic keratoses will turn into cancer. But since you can’t predict which ones will, it’s important to treat them all.
The bottom line
Actinic keratoses are scaly patches of skin caused by chronic sun damage. They can turn into skin cancer, but treatments work to prevent this. Actinic keratosis spots can be flat or raised, in a range of different colors, from pink or red to white or skin-colored. They usually appear on skin that’s been chronically exposed to the sun, like your face, scalp, ears, arms, and back of the hands.

Why trust our experts?



Images used with permission from VisualDx (www.visualdx.com).
References
American Academy of Dermatology Association. (2022). Actinic keratosis: Diagnosis and treatment.
Coulsons I., et al. (2023). Photodynamic therapy. DermNet.
Eisen, D. B., et al. (2021). Guidelines of care for the management of actinic keratosis. Journal of the American Academy of Dermatology.
Fuchs, A., et al. (2007). The kinetics of skin cancer: Progression of actinic keratosis to squamous cell carcinoma. Dermatologic Surgery.
Marques, E., et al. (2023). Actinic keratosis. StatPearls.
Oakley, A., et al. (2016). Seborrhoeic keratosis. DermNet.
Skin Cancer Foundation. (2024). Actinic keratosis overview.
Skin Cancer Foundation. (2024). Actinic keratosis risk factors.
Skin Cancer Foundation. (2024). Actinic keratosis treatment.
Venosa, A. (2023). Is actinic keratosis skin cancer? What you need to know about this common condition. Skin Cancer Foundation.